For millions of people, the simple act of walking up stairs, standing from a chair, or even tying their shoes has become a daily struggle. This isn’t just aging-it’s osteoarthritis. Often dismissed as "wear and tear," osteoarthritis is a complex disease that doesn’t just eat away at cartilage. It changes the entire joint-bone, ligaments, even the lining inside the joint. And while it can’t be cured, it can be managed. Realistically. Effectively. Without relying only on pills that hurt your stomach.
What’s Really Happening Inside Your Joint?
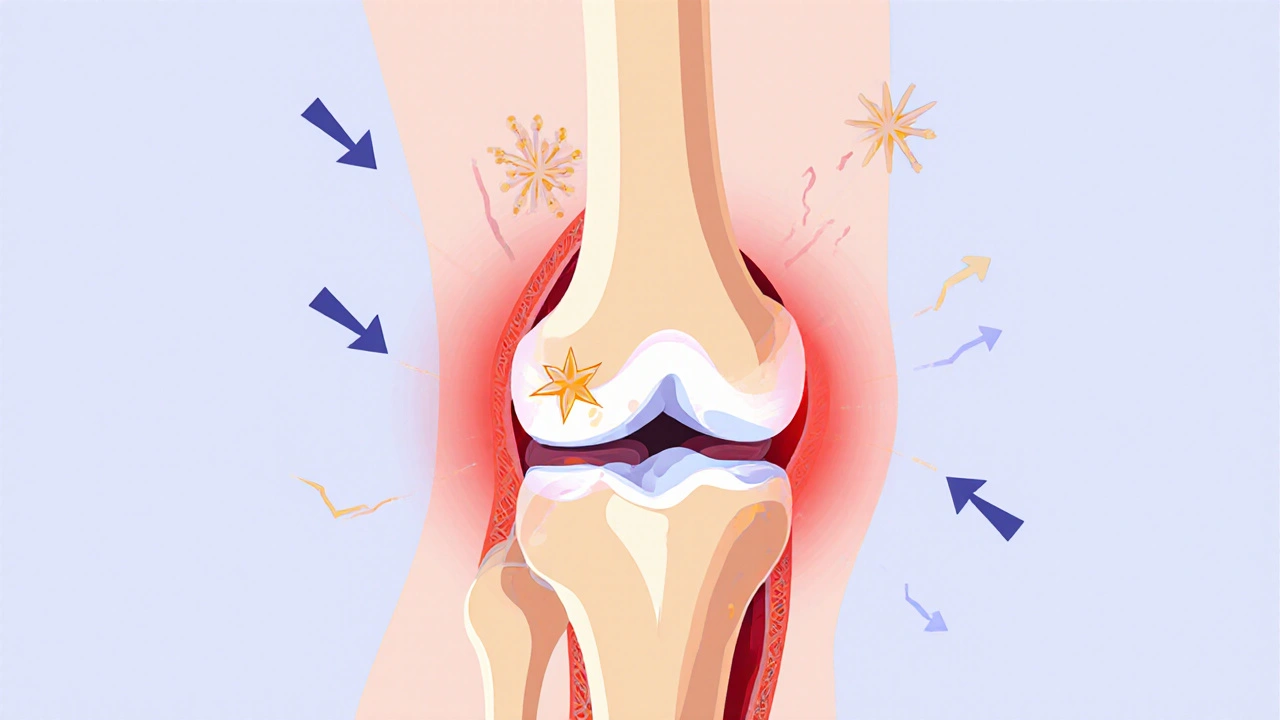
Your joints aren’t just bones rubbing together. They’re surrounded by cartilage-a smooth, rubbery cushion that lets bones glide without friction. In osteoarthritis, that cushion breaks down. Not because you’ve used it too much, but because the body’s repair system has stopped keeping up. Tiny cracks form in the cartilage. Chondrocytes, the cells that maintain cartilage, go into overdrive trying to fix it, but they end up making more inflammation than healing. Over time, the cartilage thins, bones start to grind, and bone spurs (osteophytes) grow around the joint edges. The synovial fluid that normally lubricates the joint gets thinner. Ligaments stretch. Fat pads around the joint swell. It’s not just one thing breaking-it’s the whole system falling out of balance.Where Does It Usually Show Up?
Not all joints are equally affected. Knees are the most common, hitting about 60% of people with OA. Hips follow at 30%, then hands and the spine. What’s interesting is how uneven it is. You might have severe OA in your right knee but barely any in the left. That’s because it’s not just about age-it’s about how you’ve used your body. A construction worker with years of kneeling is far more likely to have knee OA than someone who sits at a desk. Women are more likely to develop knee and hand OA, while men tend to get worse hip OA. And it’s not just older people. One in five adults over 45 have doctor-diagnosed OA. It’s not normal aging. It’s a disease you can influence.How Is It Different From Other Arthritis?
If you’ve heard of rheumatoid arthritis (RA), you might think they’re the same. They’re not. RA is an autoimmune disease-your immune system attacks your joints. OA? It’s mechanical and biological. Pain from OA gets worse when you move, and it improves when you rest. With RA, pain is often worse in the morning and gets better after you’ve been moving for a while. Gout comes on suddenly, with red, hot, swollen joints-usually the big toe. OA creeps in slowly. You might notice stiffness after sitting for a while, or a clicking sound in your knee. At first, it’s just annoying. Then it becomes limiting. And because it’s slow, many people wait years before seeing a doctor. By then, X-rays show significant damage. That’s the problem: we’re diagnosing it too late. New research is looking for blood markers that could spot OA years before symptoms start.Why Pain Management Isn’t Just About Pills
Painkillers like ibuprofen or naproxen (NSAIDs) are common, but they come with risks. About one in three people stop taking them because of stomach upset, kidney strain, or high blood pressure. And they don’t stop the joint from breaking down-they just mask the pain. That’s dangerous. If you can’t feel the pain, you might push your joint too hard, making things worse. The real solution? A three-part plan: movement, weight control, and education.Move-Even When It Hurts
The biggest myth about OA is that you should rest. Rest makes muscles weaker, joints stiffer, and pain worse. Movement is medicine. Land-based exercise-like walking, cycling, or water aerobics-is proven to reduce pain by 40% in 12 weeks. The Arthritis Foundation recommends 45 minutes, three times a week. You don’t need to run marathons. Just keep moving. Strength training matters too. Stronger quadriceps (thigh muscles) take pressure off the knee. One study showed that people who did leg exercises three times a week for six months reduced their knee pain by half. Physical therapy isn’t a luxury-it’s essential. Six to eight sessions with a certified therapist can teach you how to move safely, protect your joints, and avoid movements that worsen pain.
Weight Loss: The Most Effective Treatment
Losing weight isn’t just about looking better-it’s about saving your joints. Every pound you lose takes four pounds of pressure off your knees. That means if you drop 10 pounds, you’re removing 40 pounds of stress from each knee. A 2022 Arthritis Foundation survey found that 72% of people who lost 10% of their body weight saw major improvements in pain and mobility. You don’t need to lose 50 pounds. Just 10. That’s enough to make a real difference. Combine it with exercise, and the results are even better. People who lost weight and exercised had 50% less pain than those who only took pills.What About Injections and Surgery?
Corticosteroid injections into the knee can give relief for several weeks-up to 50% pain reduction in many cases. They’re great for flare-ups, but not for long-term use. Too many injections can damage cartilage over time. Hyaluronic acid shots (lubrication injections) have mixed results. Some people feel better; others don’t. The FDA approved a new drug called tanezumab in 2023. It targets nerve growth factor and reduces pain 35% more than NSAIDs. But it’s only for moderate-to-severe cases, and it’s not available everywhere yet. Surgery-like knee replacement-is the last step. It’s highly effective, but it’s major. Only about 1 in 10 people with knee OA ever need it. Most can manage with the basics: movement, weight control, and smart habits.What Doesn’t Work (And What’s Still Unproven)
Glucosamine and chondroitin supplements? Large studies show they don’t help more than a placebo. Same with collagen powders. They’re big business, but the science isn’t there. Stem cell therapy? There are over 380 clinical trials going on right now. Some early results look promising, but it’s still experimental. No major medical group recommends it yet. PRP (platelet-rich plasma) injections? Mixed results. Some people feel better; others don’t. Don’t spend thousands on unproven treatments. Focus on what works: exercise, weight loss, and joint protection.Living With OA: Daily Strategies That Help
Small changes make a big difference. Use a cane or walker if your knee gives out. Wear supportive shoes with cushioned soles. Avoid high heels. Use jar openers, reachers, and ergonomic tools to protect your hands. Take breaks during long tasks. Sit instead of standing when you can. Apply heat for stiff joints, ice for swollen ones. Sleep on a firm mattress. Use pillows to support your knees or hips. These aren’t gimmicks-they’re practical tools that keep you moving and reduce strain.
Why So Many People Are Struggling
The system isn’t working well for most people. The average wait time to see a rheumatologist is over eight weeks. Many primary care doctors don’t have time to teach joint protection techniques. Insurance often won’t cover physical therapy beyond a few visits. And employers? Only 1 in 3 know how to accommodate someone with OA. The CDC says 43% of people with arthritis limit their work activities because of pain. That’s not just personal-it’s economic. OA costs the U.S. $140 billion a year in medical bills and lost productivity. We’re treating the symptoms, not the cause. And the cause? Obesity and inactivity. Forty-two percent of U.S. adults are obese. Only 23% meet physical activity guidelines. Until we fix those, OA will keep rising.The Future: Early Detection and Prevention
The good news? We’re getting better at catching OA early. Researchers are testing blood tests that can detect joint breakdown before pain starts. In five years, we might be able to identify people at risk and stop OA before it begins. Community programs like the CDC’s "Active People, Healthy Nation" are bringing free exercise classes to parks and community centers across all 50 states. These aren’t fancy labs-they’re simple, accessible, and working. People who join these programs cut their pain by 40% and improved their daily function by 30%. You don’t need a miracle. You need to move, lose weight if needed, and learn how to protect your joints.What You Can Do Today
Start small. Walk 10 minutes a day. Add 5 minutes every week. Swap soda for water. Cut out one sugary snack. Do two leg lifts while sitting in your chair. Talk to your doctor about a referral to physical therapy. Ask about a weight management program. Don’t wait for the pain to get worse. Osteoarthritis doesn’t get better on its own-but it doesn’t have to get worse, either. The tools are there. You just need to use them.Is osteoarthritis the same as rheumatoid arthritis?
No. Osteoarthritis is caused by mechanical wear and biological changes in the joint, while rheumatoid arthritis is an autoimmune disease where the body attacks its own joints. OA pain gets worse with activity and improves with rest. RA pain is often worse in the morning and improves with movement. RA can affect organs beyond joints and requires different treatments like immunosuppressants.
Can osteoarthritis be reversed?
Currently, no treatment can fully reverse cartilage damage. But you can slow or even stop its progression. Losing weight, staying active, and protecting your joints can prevent further breakdown. In some cases, early intervention can lead to symptom improvement that feels like reversal-even if the structure hasn’t fully healed.
Do I need an X-ray to diagnose osteoarthritis?
Doctors often use X-rays to confirm OA, especially if symptoms are unclear or severe. But you don’t always need one. Many people are diagnosed based on symptoms-joint pain worsened by activity, stiffness after rest, and reduced range of motion. X-rays show structural damage, but they don’t always match how much pain you feel. Some people have severe X-ray changes with little pain, and others have mild changes with severe pain.
Are joint injections safe for long-term use?
Corticosteroid injections can be very effective for flare-ups, but they’re not meant for regular, long-term use. Too many injections (more than 3-4 per year) can weaken cartilage and surrounding tissue. Hyaluronic acid injections have limited evidence of long-term benefit. Always discuss frequency and risks with your doctor. They’re a tool for short-term relief, not a cure.
Can I still exercise with osteoarthritis?
Yes-and you should. Exercise is one of the most effective ways to reduce OA pain and improve mobility. Low-impact activities like walking, swimming, cycling, and strength training help. Avoid high-impact sports like running or jumping if your knees or hips are affected. Start slow, listen to your body, and work with a physical therapist to design a safe routine. Movement keeps muscles strong, joints flexible, and pain under control.
What’s the best diet for osteoarthritis?
There’s no single "OA diet," but eating to manage weight and reduce inflammation helps. Focus on whole foods: vegetables, fruits, lean proteins, nuts, seeds, and fatty fish like salmon. Avoid sugary drinks, processed snacks, and excessive red meat. Omega-3 fatty acids from fish or flaxseed may help reduce inflammation. Staying hydrated also supports joint lubrication. The goal isn’t to cure OA-it’s to support your body’s ability to heal and move.
Will I eventually need a joint replacement?
Not necessarily. Only about 10% of people with knee OA eventually need surgery. Most manage well with lifestyle changes, physical therapy, and pain management. Joint replacement is considered when pain severely limits daily life and other treatments have failed. It’s highly successful, but it’s major surgery with a recovery period. The goal is to delay it as long as possible through proactive management.

Jeremy Samuel
lol osteoarthritis my ass. i’ve been walking 10k steps a day for 15 years and my knees still feel like wet cardboard. its not wear and tear its just your body giving up. they should just admit we’re all gonna turn into creaky robots by 50.
Destiny Annamaria
YESSS this is SO TRUE!! I lost 12 lbs last year and my knees literally stopped screaming at me. I started doing water aerobics at the rec center and now I’m dancing in my kitchen like a maniac 😭💃 No pills. No magic. Just movement and less sugar. You got this!
Ron and Gill Day
This is the same tired propaganda pushed by Big Pharma and the Arthritis Foundation. Exercise? Weight loss? Please. If it were that simple, why is OA the #1 cause of disability in the US? The real issue is that the medical industrial complex profits from chronic pain. They don’t want you healed. They want you on NSAIDs for life.
Alyssa Torres
I’m crying right now because this article spoke to me. My mom had OA and she thought she just had to suffer. I got her into PT and now she’s gardening again. It’s not about being young. It’s about being stubborn. You can still live. You just have to choose how. I’m so proud of you all who are trying.
Summer Joy
glucosamine is a scam but they still sell it like it’s holy water 💀 and don’t even get me started on stem cells. i paid $8k for one injection and now my knee looks like a raisin. the system is rigged. 🤡
Aruna Urban Planner
The biomechanical load distribution in OA is often underestimated. Synovial fluid viscosity reduction coupled with altered proprioceptive feedback creates a feedback loop of degeneration. Interventions targeting neuromuscular efficiency show higher long-term efficacy than pharmacological suppression. Evidence-based kinesiology remains underutilized in primary care settings.
Nicole Ziegler
i started walking with my dog every morning and now i can tie my shoes without crying 🐶❤️ sometimes the small things are the biggest wins
Bharat Alasandi
bro i was skeptical but i did 20 squats a day for 3 months and my knee pain dropped 70%. no joke. its not about being jacked, its about being consistent. also drink more water. your joints are 70% water lmao
Kristi Bennardo
This article is dangerously misleading. The CDC data cited is cherry-picked. The true prevalence of OA is far higher than reported, and the effectiveness of exercise is overstated for those with advanced degeneration. Many patients are left with no viable options but opioids or surgery. This is not empowerment-it’s victim-blaming disguised as advice.
Shiv Karan Singh
you think weight loss fixes it? my uncle was 200 lbs and had OA for 20 years. he lost 80 lbs and still couldn't walk. the real problem? your genes. and the doctors know it. they just don't wanna tell you.
Ravi boy
i been doing yoga and drinking turmeric tea and my hip dont hurt as much. also i dont own a car so i walk everywhere. maybe its not the medicine its the lifestyle. just saying
Matthew Karrs
They’re hiding the truth. OA isn’t natural. It’s caused by glyphosate in our food, fluoridated water, and 5G radiation. The FDA banned the real cure in 1983. If you’re not taking MMS or colloidal silver, you’re being played.
Matthew Peters
I used to think movement was torture until I tried tai chi. Now I do it every morning before coffee. The pain didn’t vanish, but it stopped ruling me. I didn’t know you could retrain your body like that. Mind blown.
Liam Strachan
I’m from the UK and we’ve got free physio on the NHS. It’s not perfect, but it’s there. I wish more people knew that help like this exists. You don’t need to suffer alone. Just ask. It’s okay to need help.
Gerald Cheruiyot
The real tragedy isn’t the cartilage loss. It’s the cultural belief that aging means surrender. We’ve turned a biological process into a moral failing. The body doesn’t break because you’re weak. It breaks because we stopped listening. We built a world that rewards motionless productivity and then wonder why we’re all falling apart.