ACE Inhibitor & Renal Stenosis Risk Checker
Select the clinical scenario to see how ACE inhibitors (ACEIs) affect kidney filtration pressure.
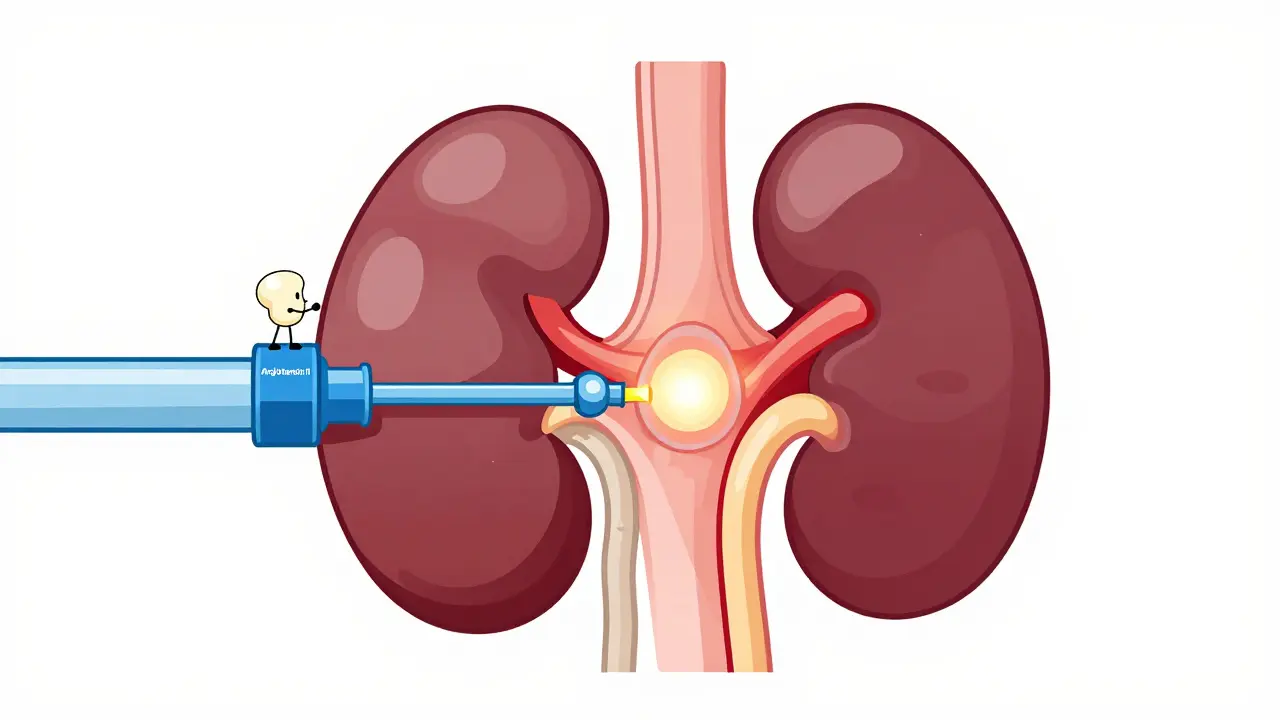
Imagine your kidneys as a high-pressure filtration system. To work properly, they need a very specific amount of pressure inside their tiny filters, known as glomeruli. Now, imagine the pipe leading into that system is narrowed-that's Renal Artery Stenosis is a condition where the arteries that carry blood to the kidneys narrow, reducing blood flow. In this scenario, the body has a brilliant backup plan to keep the filters running. It uses a hormone called Angiotensin II to tighten the "exit pipe" (the efferent arteriole), which builds up pressure behind the clog and keeps the kidney filtering waste. Everything is balanced, albeit precariously.
Then comes the medication. ACE Inhibitors (ACEIs) are pharmaceutical agents that block the conversion of angiotensin I to angiotensin II, primarily used to lower blood pressure and protect the heart. While they are lifesavers for millions of people with hypertension or heart failure, they act like a wrecking ball to that specific backup plan in patients with severe artery narrowing. By removing Angiotensin II, the "exit pipe" flops open. The pressure inside the kidney drops instantly, filtration stops, and the patient can slide into acute renal failure in a matter of days.
The Danger Zone: Bilateral vs. Unilateral Stenosis
Not every narrowed artery is a deal-breaker for these meds. The critical danger happens when there is no "healthy" kidney to pick up the slack. This is why the ACE Inhibitors contraindication is so specific. If you have Bilateral Renal Artery Stenosis (narrowing in both kidneys) or a single functioning kidney that is stenotic, you are in the danger zone. Without a healthy kidney to maintain overall filtration, blocking that pressure-regulating hormone can lead to a catastrophic drop in the Glomerular Filtration Rate (GFR).
On the flip side, if you have unilateral stenosis-meaning only one kidney is narrowed and the other is perfectly healthy-the risks are much lower. Research, including a follow-up analysis of the ASTRAL trial, showed that people with unilateral stenosis didn't see a significant difference in kidney function decline when using ACEIs compared to those who weren't. The healthy kidney simply does the heavy lifting, making the medication much safer in that specific context.
How the Kidney "Crash" Actually Happens
To understand why the kidneys fail, we have to look at the plumbing. In a stenotic kidney, the blood pressure arriving at the glomerulus is too low. To compensate, the kidney releases renin, which eventually creates Angiotensin II. This hormone increases the resistance of the efferent arteriole by about 37.5% in stenotic kidneys. This is essentially like putting a thumb over the end of a garden hose to increase the pressure inside the hose.
When you introduce a drug like Lisinopril or Ramipril, you remove that "thumb." The efferent arteriole dilates, and the internal pressure drops by 25-30%. Suddenly, the kidney can no longer push fluid through the filter. Clinically, this shows up as a sharp rise in serum creatinine-usually more than 30%-within about a week of starting the drug. This isn't a slow decline; it's an abrupt functional collapse.
| Stenosis Type | Mechanism | Clinical Outcome | Risk Level |
|---|---|---|---|
| Bilateral (Both Sides) | Global loss of efferent resistance | Acute Renal Failure / GFR Drop | High (Contraindicated) |
| Unilateral (One Side) | One kidney fails, other compensates | Stable overall kidney function | Low/Moderate |
| Solitary Kidney (Stenotic) | No backup filtration source | Acute Renal Failure | High (Contraindicated) |
Spotting the Red Flags and Screening
How do doctors avoid this mistake? They look for specific "red flags" before prescribing. High-risk patients usually fit a few of these descriptions: they have hypertension that is suddenly very hard to control, unexplained kidney impairment, or a "bruit" (a swooshing sound) heard when a doctor listens to the abdomen with a stethoscope. In these cases, a Renal Artery Duplex Ultrasound is the gold standard for screening. It's highly accurate, with about 86% sensitivity for detecting significant narrowing.
Even with these warnings, mistakes happen. Some studies have found that over 20% of patients with known bilateral stenosis were still prescribed these drugs in primary care. This is why the monitoring phase is so critical. Guidelines from NICE suggest checking renal function and potassium levels before starting the drug, and then again about 10 days after the first dose. If the creatinine jumps by 30% or more in those two weeks, it's a massive warning sign that bilateral stenosis might be present.

The ARB Misconception
A common mistake is thinking that Angiotensin Receptor Blockers (ARBs), like Losartan, are a safe alternative. They aren't. While ACE inhibitors stop the *production* of Angiotensin II, ARBs block the *receptors* that the hormone binds to. The result is the same: the efferent arteriole dilates, the pressure drops, and the kidney stops filtering. If a patient has acute renal failure from an ACE inhibitor, switching to an ARB is not a solution; it's just another way to achieve the same negative result.
Recovery and Long-term Outlook
The good news is that this type of kidney damage is usually reversible. If the drug is stopped quickly, the body can resume its natural pressure-regulation process, and the GFR typically bounces back. However, there is a ticking clock. If the kidney stays under-perfused (hypoperfused) for more than 72 hours, the damage can become permanent. This makes the "10-day check-up" mentioned in clinical guidelines a literal lifesaver.
Why are ACE inhibitors usually good for kidneys but bad here?
In most people, ACE inhibitors protect the kidneys by lowering overall pressure and reducing "wear and tear." However, in someone with renal artery stenosis, the kidney is *already* struggling for pressure. The drug removes the only mechanism (Angiotensin II) that was keeping the filtration pressure high enough to work. It's the difference between lowering a high-pressure hose to a safe level versus turning off a hose that was barely trickling.
Can I take an ACE inhibitor if I only have one kidney?
It depends. If your single kidney is healthy, ACE inhibitors are often used. But if that single kidney has renal artery stenosis, the medication is strictly contraindicated because there is no second kidney to maintain your body's filtration needs if the first one fails.
What are the symptoms of this reaction?
You might not feel anything at first. The "reaction" is a functional failure inside the kidney. The primary sign is a spike in serum creatinine levels on a blood test. Some people might notice decreased urine output or swelling (edema) as waste products and fluids build up in the blood.
Is the damage permanent?
In most cases, the deterioration is reversible if the medication is discontinued promptly. However, if the kidney is deprived of adequate blood flow and pressure for longer than 72 hours, there is a risk of permanent tissue damage and chronic kidney disease.
What should I ask my doctor if I'm concerned?
Ask if your renal function should be monitored 10-14 days after starting the medication. If you have a history of severe high blood pressure or vascular disease, ask if a duplex ultrasound is necessary to rule out bilateral stenosis before beginning therapy.

Toby Sirois
Pretty basic stuff. Anyone who actually knows medicine knows that ARBs are basically the same thing as ACE inhibitors in this context. It's honestly wild that some people still think switching to Losartan is a magic fix when the whole problem is the efferent arteriole dilation. Just get a duplex ultrasound and stop guessing with your health.
Brady Davis
Oh great, so basically my doctor could accidentally nuke my kidneys in ten days while I'm just sitting there feeling "fine." Absolutely thrilling!
Alexander Idle
The sheer audacity of primary care physicians prescribing these to people with bilateral stenosis is just a cinematic tragedy of errors. I mean, imagine the chaos in the clinic when the creatinine levels hit the ceiling. It's a total disaster waiting to happen, and honestly, the system is just crumbling around us while we're all pretending everything is Gucci. I can't even with this level of incompetence in the medical field. It's like they're playing a game of Russian Roulette with our renal arteries. Truly a masterclass in how to fail at basic pharmacology. I'm practically shaking just thinking about the lack of screening. Absolute madness.
Vivek Hattangadi
This is a really helpful breakdown of the mechanism! It's so important to keep an eye on those blood tests after starting new meds. Maybe we can suggest a checklist for patients to bring to their 10-day follow-up to make sure the creatinine check actually happens!
Daniel Trezub
Actually, the ASTRAL trial data is often misinterpreted. While unilateral stenosis is generally safer, you can't just ignore the potential for rapid progression in some patients. It's not as black and white as the table makes it look, but hey, it's a decent summary for beginners.
Sarabjeet Singh
Stay positive everyone, just keep the communication open with your doctors.
Rupert McKelvie
It is quite reassuring to know that the damage is usually reversible if caught within those first few days. The 10-day monitoring window is a great safety net for patients.
charles mcbride
I believe this information will empower many patients to have more proactive conversations with their healthcare providers. It is wonderful to see the complex relationship between blood pressure medication and renal health explained so clearly.